
The System Is Failing: 5 Shocking Truths About Mental Healthcare for Black Communities in the UK
Introduction: More Than Just a Headline
In the wake of the global Black Lives Matter movement and the harsh light the COVID-19 pandemic cast on systemic inequality, conversations about racial justice and mental health have become more widespread than ever. We have begun to acknowledge, as a society, that experiences of racism have profound psychological consequences. But beyond this general awareness, what are the hidden, systemic realities that Black individuals face when they seek mental health support in the UK?
This article moves beyond the headlines to reveal the deep-seated inequalities embedded within the very foundations of psychological therapy. While this article uses terms like "Black communities" and "BME" for clarity, we acknowledge these are broad categories encompassing many diverse experiences and identities. Drawing on recent research, we will uncover five of the most impactful truths about the barriers, biases, and historical injustices that shape mental healthcare experiences. These are not isolated incidents but patterns that reveal a system in urgent need of transformation.
--------------------------------------------------------------------------------
1. Psychiatry Invented Racist "Disorders" to Justify Slavery
Long before Western psychiatry offered healing, some of its pioneers were inventing "disorders" to justify the brutal institution of slavery. This history is not an academic footnote; it is the toxic root of a well-earned mistrust that persists today. The American Psychiatric Association (APA) only issued a formal apology for its support of structural racism in January 2021, a legacy with racist roots dating back to the 1700s.
During this era, white psychiatrists created "drapetomania," a supposed mental illness whose primary symptom was an enslaved person’s desire to escape bondage. This diagnosis pathologized the natural human impulse for freedom, with medically prescribed "treatments" that included severe beatings and the amputation of toes. In a grotesque display of dehumanization, enslaved Black people were even used as payment for the psychological treatment of whites. Other theories, like "negritude," falsely claimed that the skin color of Black people was a form of leprosy. This history shows how the tools of mental health were weaponized to uphold oppression, establishing a foundation of harm rather than help.
This medical dehumanization was directly mirrored by an economic system that treated Black people not as humans, but as assets.
2. Slave Owners Received Billions in Compensation. The Enslaved Received Nothing.
The economic legacy of slavery continues to fuel systemic inequality in Britain. When the Slavery Abolition Act was passed in 1833, it did not lead to reparations for the people who had been enslaved. Instead, it triggered a massive compensation scheme for their oppressors.
From 1833 all the way up to 2015, the British government paid what would be equivalent to billions of pounds to slave traders and owners to compensate them for their "loss of earnings"—the human beings they had enslaved.
"From 1833 up until 2015, slave traders were in receipt of compensation (up to 17 billion pounds) for loss of earnings; slaves were considered business assets."
This staggering fact illustrates a system designed from its core to value the wealth of oppressors over the lives of the oppressed. This history of economic dehumanization laid the groundwork for a modern system that continues to devalue Black individuals, often seeing them not as people in need of care, but as problems to be managed through force.
3. Black Patients Are Under-Represented in Therapy but Over-Represented in Detention
Nowhere is the legacy of this historical bias more apparent than in the modern-day paradox of care: Black patients are ghosts in the therapy room but hyper-visible in detention. While individuals from Black Minority Ethnic (BME) backgrounds are less likely to access voluntary care, they are far more likely to be sectioned and diagnosed with severe illness.
The numbers paint a damning portrait of a two-tiered system:
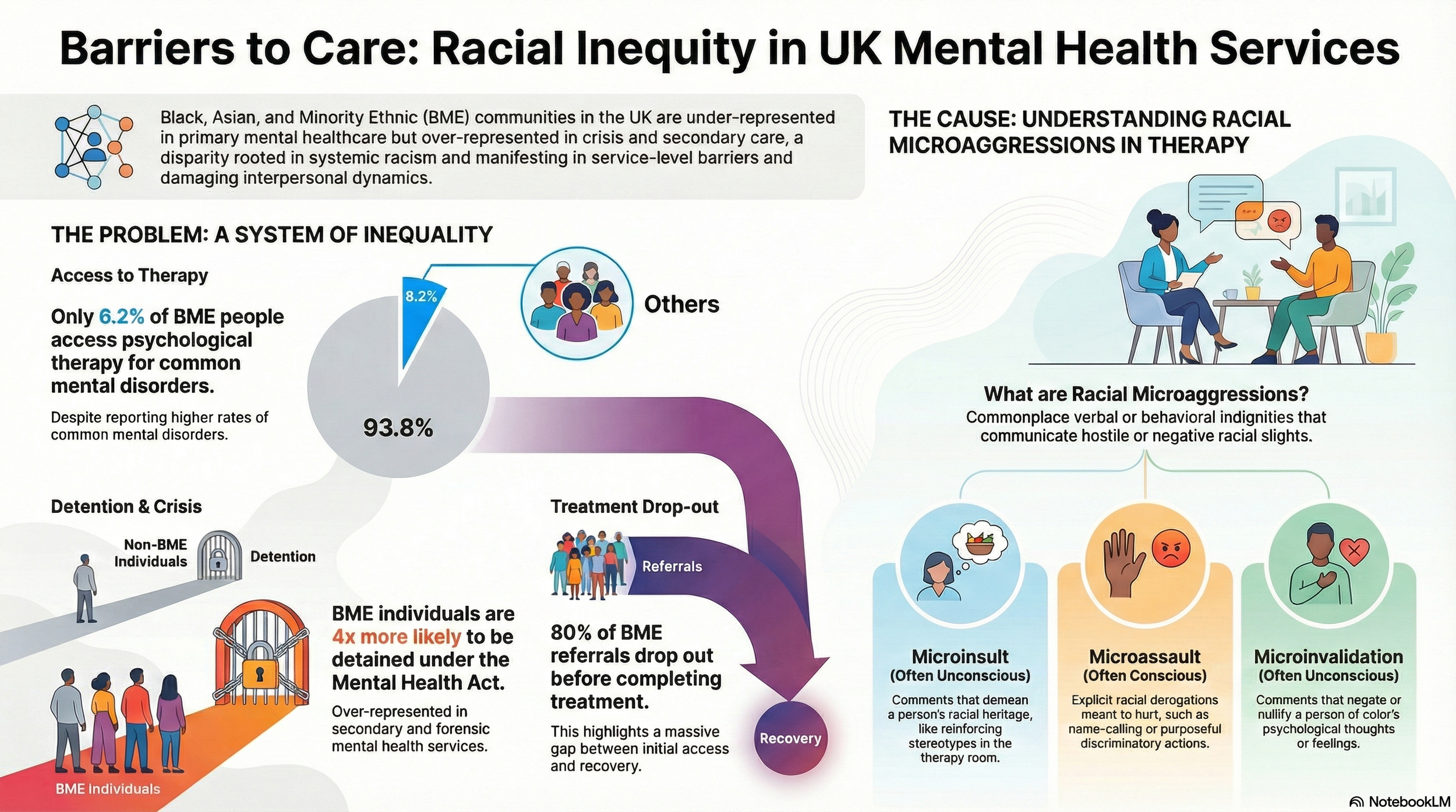
• Individuals from BME backgrounds are four times more likely to be detained under the Mental Health Act compared to the white population, encountering the system through coercion and crisis.
• Conversely, only 6.2% of BME people access psychological intervention for common mental disorders through the UK's primary, voluntary route, the Improving Access to Psychological Therapies (IAPT) programme.
This paradox means that for many Black individuals, their most significant encounter with mental health services is not one of choice or support, but of force. This dynamic reinforces the historical mistrust and positions the system as a threat, not a refuge. And for the few who do navigate the barriers to voluntary care, the sanctuary of therapy can become a site of fresh racial injury.
4. The Therapy Room Can Reinforce Daily Experiences of Racism
For the few who navigate the barriers to voluntary care, the therapy room itself—supposedly a sanctuary—can become a site of fresh racial injury. These encounters often take the form of "racial microaggressions," defined as "commonplace verbal or behavioral indignities, whether intentional or unintentional, which communicate hostile, derogatory, or negative racial slights and insults."
Research provides concrete examples of how this manifests in a therapeutic setting. In one documented case of a microinsult:
• "A white therapist references interaction within a group therapeutic setting and states that the older white middle-aged white SU [service user] contributed well, despite being positioned in between ‘two big black men’. Inferring that the white lady’s positioning implied propensity for at risk or may have made her feel threatened. Reinforcing the ‘big black and dangerous’ stereotyping."
Compounding this issue is the finding that many Cognitive Behavioural Therapy (CBT) therapists "may steer away from discussions on race." When a therapist ignores, minimizes, or perpetuates a patient's experience of racism, it invalidates their reality and destroys the therapeutic alliance. It is the ultimate betrayal, and it helps explain why so many Black patients walk away from care.
5. The Vast Majority of Black Patients Drop Out of Therapy
The cumulative weight of this systemic failure is captured in one devastating statistic: the vast majority of Black patients who seek help are ultimately driven away. A review of NHS data from the Talking Therapies Southwark (TTS) service during Q3 2019/20 provides a clear and alarming picture. In Southwark, a diverse London Borough where 25% of the population is from BME backgrounds, the attrition rate is staggering.
The data revealed that of 630 referrals from the BME community, only 145 went on to complete their treatment. This led researchers to a stark conclusion:
"This evidences that at least 80% of BME people drop out of therapy between referral, assessment and into treatment stages."
This 80% attrition rate is more than just a statistic; it is a quantifiable measure of a failed journey. It proves that even when Black individuals overcome immense barriers to ask for help, the process itself is so fraught with obstacles that most cannot see it through. It is the final, predictable outcome of a system that was never truly built for them.
--------------------------------------------------------------------------------
Conclusion: Where Do We Go From Here?
These five truths make one thing clear: these are not disparities; they are the predictable outcomes of a system designed to fail Black communities. From its racist origins to the modern-day realities of coercion, microaggressions, and abandonment, the journey from seeking help to finding healing is riddled with points of failure that disproportionately harm Black individuals.
The path forward requires more than surface-level fixes. Given that every stage of the mental health journey can inflict new harm, how do we stop trying to patch a broken system and begin to build one that is finally worthy of trust?