
Beyond the Numbers: The Hidden Barriers Holding Women Back in Medicine
In 2017, a major milestone was reached in the United States: for the first time in history, women made up the majority (50.7%) of new medical students. By 2019, they accounted for 50.5% of all medical students, cementing the idea that gender parity in medicine was finally within reach. This surface-level progress, while important, masks a much more complex and troubling reality.
Beneath the promising enrollment numbers lies a landscape of persistent, systemic barriers that prevent women from advancing at the same rate as their male colleagues. For women of color, these barriers don't just add up—they multiply and compound one another, creating a web of interlocking challenges. These are not minor hurdles; they are deep-rooted structural and psychological obstacles that create significant disparities in leadership, compensation, and daily professional life.
This article will move beyond the entry-level statistics to reveal some of the most surprising and impactful challenges that persist in academic medicine. By understanding these hidden barriers, we can see why simply opening the door is not enough to guarantee a level playing field.
The Pipeline Is Strong, But It Leaks at the Top
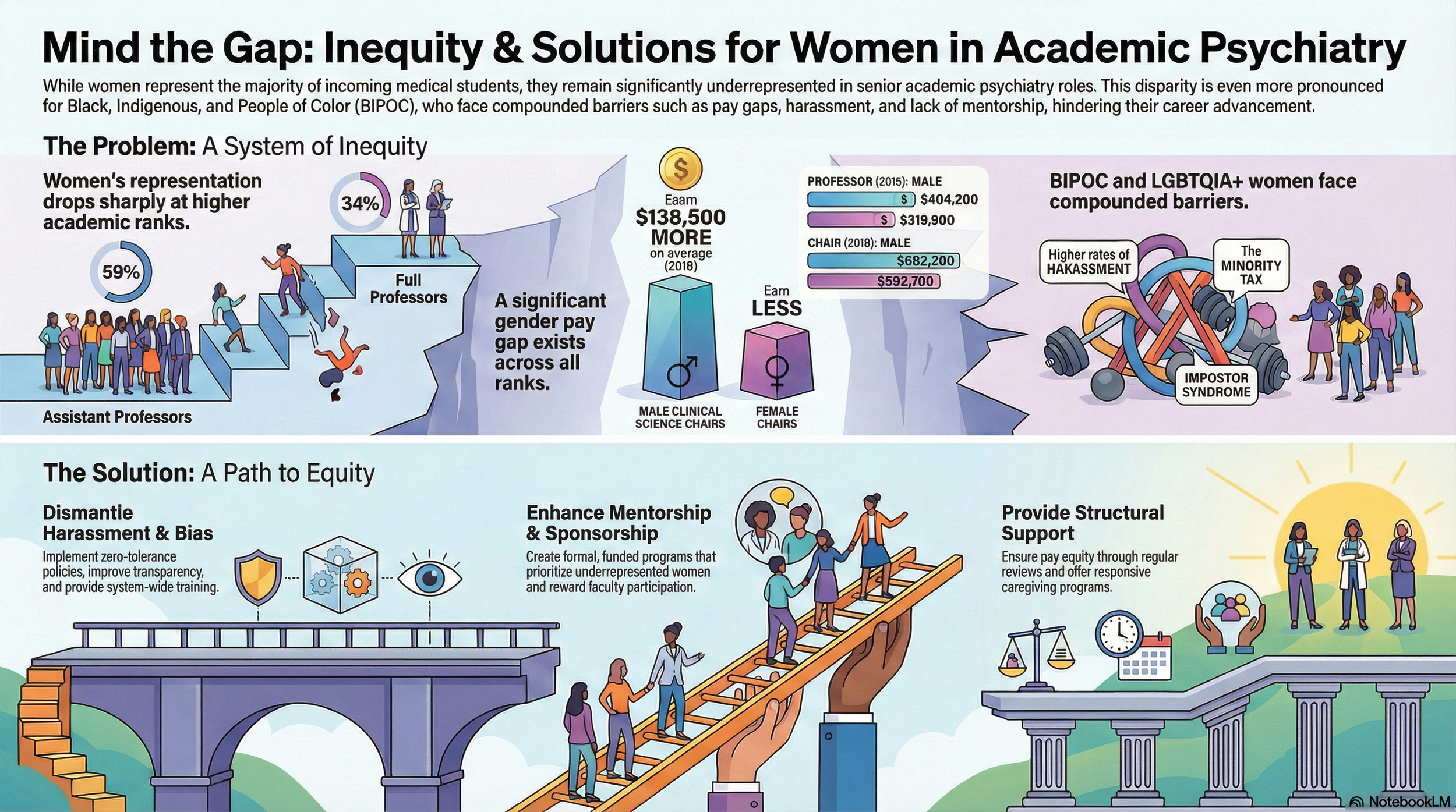
The pipeline of women entering medicine is strong, but it begins to leak significantly as careers progress. While women accounted for 50.5% of all medical students in 2019, they remain profoundly underrepresented in the highest ranks of academic medicine. The numbers reveal a stark disparity between the classroom and the boardroom.
Consider the following data points:
• Women represent only 26% of full professors among all medical faculty.
• In the field of psychiatry specifically, women account for just 34% of full professors, the majority of whom are White.
• In 2019, a mere 19% of all US medical school chairs were women.
Let that sink in: for every four men who hold the title of full professor, only one woman does. This data illustrates that while women are successfully entering the profession, they are not advancing to positions of power and influence at a proportionate rate. This lack of representation at the top isn't just about power; it's also reflected in a persistent and shocking gap in compensation.
More Than a Gap, It's a Chasm of Lost Earnings
Significant gender-based salary inequities persist across all career stages in academic medicine, and the gap is often far wider than anticipated. These disparities are not just minor differences; they represent substantial sums that accumulate over a career.
The scale of the problem is startling:
• The unadjusted average annual salary difference between male and female department chairs at public medical schools was $79,061.
• For chairs who had served for more than 10 years, this pay gap ballooned to an incredible $127,411.
This financial disparity is compounded by race, creating an even greater burden for women of color. A powerful analysis conducted between 2010 and 2013 revealed that the median physician income was 253,042forWhitemen∗∗comparedtojust∗∗152,784 for Black women. This is not simply a gap; it's a chasm. Crucially, this disparity is compounded by generations of structural racism, as Black women generally have less familial wealth than White women. The long-term consequences are severe, as less income during working years translates directly to less retirement income, social security, and pension benefits.
The Hidden Workload of the "Minority Tax"
For faculty from underrepresented backgrounds, there is an additional, often invisible, workload known as the minority tax. This isn't a financial tax, but refers to the immense, uncompensated burden of extra responsibilities placed on minoritized persons. It is a tax on time, energy, and focus that directly impacts career advancement.
This hidden labor often includes:
• Being designated as the representative spokesperson for their entire racial group.
• Being assigned to institutional diversity efforts, frequently without compensation or formal recognition.
• Mentoring a disproportionately large number of diverse students, often with inadequate institutional support.
This work is so detrimental because it is often unrecognized, uncompensated, and required of faculty members simply because of their minoritized status. The most insidious effect of this tax is that it disrupts scholarly productivity by diverting a minoritized faculty’s time away from the very activities—research, publishing, and clinical work—that are critical for promotion. This creates a direct link between this invisible labor and the leadership gap at the top.
The Psychological Toll of a Biased System
Navigating a system filled with these barriers creates a significant psychological burden. This is not a sign of individual weakness but a predictable outcome of persistent bias and discrimination. Two key phenomena that disproportionately affect women, and particularly women of color, are impostor syndrome and the "double bind."
Impostor syndrome is a pattern in which individuals doubt their abilities and live in fear of being exposed as a fraud, despite clear evidence of their success. Research shows its impact is not felt equally:
• One study revealed that 50% of female medical students were affected, compared to just 25% of male students.
• The same study found it was less prevalent among White and Asian medical students (30%) than among students of other race/ethnicities (73%).
Minoritized women also face a "double bind," a no-win scenario where they must constantly manage their visibility. They risk becoming hyper-visible for their race or gender rather than for their competence, or they can become "chronically invisible" by trying to blend into the dominant culture, thereby silencing their own contributions. This stressful balancing act is exacerbated by the daily experience of microaggressions, which researchers define as:
"brief and commonplace daily verbal, behavioral and environmental indignities, whether intentional or unintentional, that communicate hostile, derogatory, or negative racial slights and insults to the target person or group"
Ultimately, these psychological challenges are not personal failings. They are the direct result of navigating a system that constantly questions one's competence, value, and belonging.
Looking Beyond the Numbers
The fact that more women are entering medical school is a positive first step, but it is only that—a first step. Achieving true equity requires us to see how these barriers create a self-reinforcing cycle. A lack of representation in leadership perpetuates unequal pay structures and devalues the invisible "minority tax" labor. This, in turn, fosters a biased environment that creates profound psychological distress, which makes it even harder for the next generation of women to reach those leadership positions.
To create a truly equitable system, we must commit to dismantling this entire cycle. We must address the stark disparities in leadership, confront the shocking reality of the pay gap, recognize and compensate invisible labor, and understand that the psychological distress experienced by many women is a systemic failure, not a personal one.
Knowing these deep-rooted challenges exist, what is the single most important action that medical institutions should take to move from performative statements to genuine, structural change?