
The Unlikely Weapon Against Racism in Medicine: Cognitive Behavioral Therapy
We place immense trust in medical professionals, believing their decisions are guided by objectivity and evidence. Yet, persistent racial health disparities tell a different story, suggesting a deeper, more systemic problem is at play. Even with the best intentions, the outcomes for patients of color often lag behind, forcing a difficult question: What are we missing in the fight for medical equity?
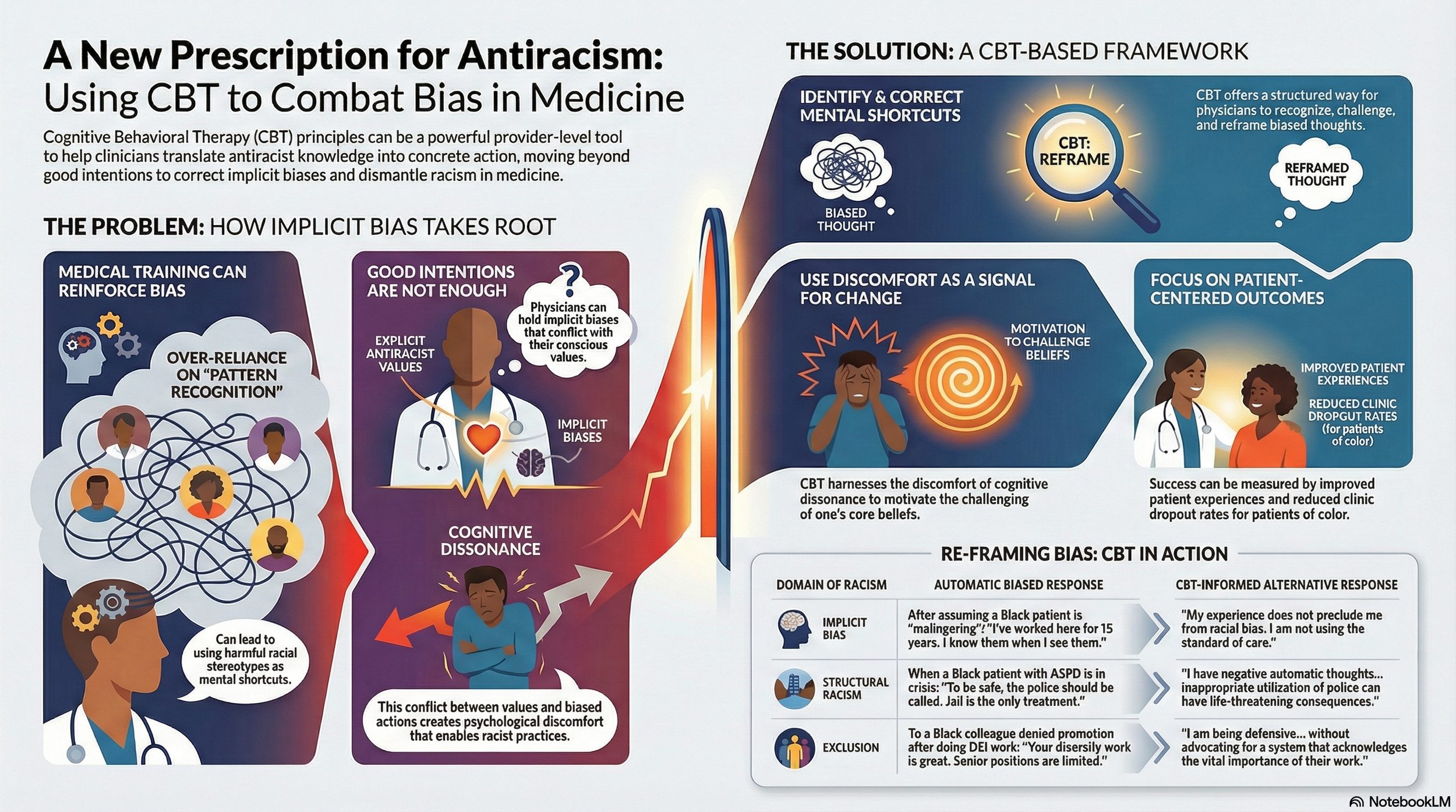
The answer may be found in a surprising place: the very mental shortcuts that make doctors efficient. A new viewpoint from psychiatric experts proposes that these shortcuts can also perpetuate unconscious bias. The suggested solution is equally unexpected: applying the principles of Cognitive Behavioral Therapy (CBT), a common form of psychotherapy, to help providers recognize and unlearn the harmful thought patterns that contribute to inequitable care.
1. A Doctor's "Pattern Recognition" Can Reinforce Racial Stereotypes
Medical education heavily prioritizes a skill called "pattern recognition"—a non-analytic process where clinicians use combinations of signs and symptoms to quickly suggest a diagnosis. While this mental shortcut is often essential for efficient care, it carries a significant risk. Under stress or time pressure, it can cause physicians to revert to ingrained racial stereotypes.
This dynamic is illustrated in a clinical scenario where an attending physician reviews the chart of a 50-year-old Black patient with "altered mental status." Noting a history of encounters for "malingering," the physician dismisses the patient, stating, "I know malingerers when I see them." This is a classic example of the defensiveness the CBT framework aims to address. The snap judgment, based on stigmatizing language, leads to a missed diagnosis, and the patient is later hospitalized for respiratory failure from COVID-19. A CBT-informed approach encourages a physician to challenge that initial, defensive thought process:
"I am being defensive. My 15 years of work experience does not preclude me from racial bias. Objectively, I am not using the standard of care to evaluate altered mental status in this Black patient. Stigmatizing language in the chart can negatively influence my attitudes towards patients and adversely affect management."
2. Good Doctors Can Hold Unconscious Biases
A central challenge in addressing racism in medicine is cognitive dissonance: the state where a physician can hold conscious antiracist attitudes but still act on implicit racial biases. When this conflict between belief and behavior isn't resolved, it enables and supports racist medical practices. However, research by social psychologist Patricia Devine and her colleagues suggests this very dissonance can be a powerful motivator for change. Their "Breaking the Prejudice Habit" intervention found that when individuals become aware of the contradiction, the resulting psychological discomfort motivates them to seek out information or perform behaviors to reduce prejudice expression. This dynamic is starkly illustrated in a psychiatric setting where a supervisor's automatic thoughts lead to a harmful outcome.
Consider a scenario where a supervisor advises a psychiatry resident to call the police on a 30-year-old Black patient with a history of antisocial personality disorder (ASPD) who was recently released from prison and is allegedly "being threatening." The supervisor's automatic thought is that "jail is the only treatment for ASPD." This individual bias directly perpetuates the broader structural problem of the "mental health criminalization in Black patients," and ultimately leads to the patient being injured while restrained by police. Recognizing the dissonance between a desire to help and a harmful, stereotype-driven action requires challenging those automatic thoughts:
"I am being defensive. I have negative automatic thoughts about antisocial behavior and legal history in Black patients, which I am not reconciling with the ongoing crisis of mental health criminalization in Black patients. Inappropriate utilization of police can have life-threatening consequences.”
3. Cognitive Behavioral Therapy (CBT) Could Be a Tool for Change
While promising, CBT-based frameworks for antiracism have not been commonly developed for medical professionals. The core hypothesis of the viewpoint article is that these frameworks, already familiar to many in mental health, can be adapted to help physicians implement antiracism. This approach teaches clinicians to systematically identify, react to, and correct the problematic mental shortcuts that turn antiracist knowledge into inaction. Crucially, a CBT-based framework can also help providers manage the defensive responses that naturally arise when their biases and actions are challenged.
This defensiveness isn't just individual; it can be institutional. In one example, a 40-year-old Black psychiatrist at an academic medical center is tasked with singlehandedly running the department's diversity programs. After being denied a promotion, she voices concern to a senior faculty member that the work environment is discriminatory. The senior colleague offers only tepid praise and avoids the core issue. The authors of the viewpoint note that this kind of passivity can stem from a systemic issue: because Black physicians are profoundly underrepresented in medicine, it creates an insular community of healthcare leaders who are prone to defensiveness when confronted with racial challenges. In the scenario, the Black psychiatrist resigns, leaving the department with no psychiatrists of color. A CBT-based mindset could challenge this institutional passivity:
"I am being defensive. I am tepidly praising my colleague’s work, without advocating for a tenure and promotion system that acknowledges the vital importance of their work, or acknowledging that health care environments are discriminatory to physicians of color, creating barriers to advancement."
Rewiring Our Approach to Medical Equity
While large, system-level interventions are essential to dismantle structural racism in healthcare, they are not the only piece of the puzzle. The fight for equity also requires tools that work at the provider level, empowering individual clinicians to translate their knowledge of antiracism into consistent, moment-to-moment antiracist action. A framework based on Cognitive Behavioral Therapy offers a promising new pathway to bridge that gap.
By applying therapeutic principles to clinical practice, we can help medical professionals challenge their own automatic thoughts and defensive reflexes. This raises a compelling question for the future: If the same therapeutic tools that help individuals challenge their own maladaptive thoughts can be applied to medicine, what other deep-seated societal problems could benefit from a cognitive shift?