
The 4 Hidden Mindsets Sabotaging Health Equity, According to a 17-Year Study
Introduction: The Stubborn Persistence of Inequity
Despite decades of significant resources, research, and dedicated effort aimed at eliminating health and healthcare inequities in the United States, they stubbornly persist, a reality brought into stark relief by the COVID-19 pandemic. We have invested in programs, collected data, and launched countless initiatives, yet the gaps in health outcomes between different racial and ethnic groups remain. This lack of progress forces a difficult question: What if the problem isn't just a lack of effort, but something deeper?
What if the most significant barriers are the deeply embedded, unexamined assumptions in our own thinking? These aren't theoretical concerns. They are the hard-won lessons from a 17-year national program funded by the Robert Wood Johnson Foundation that set out to find solutions. Through a rigorous process of action and reflection (praxis), the program uncovered powerful and surprising lessons about why progress stalls. This article distills the four most surprising psychological takeaways from their journey, revealing the hidden mindsets that can sabotage even the most well-intentioned efforts.
--------------------------------------------------------------------------------
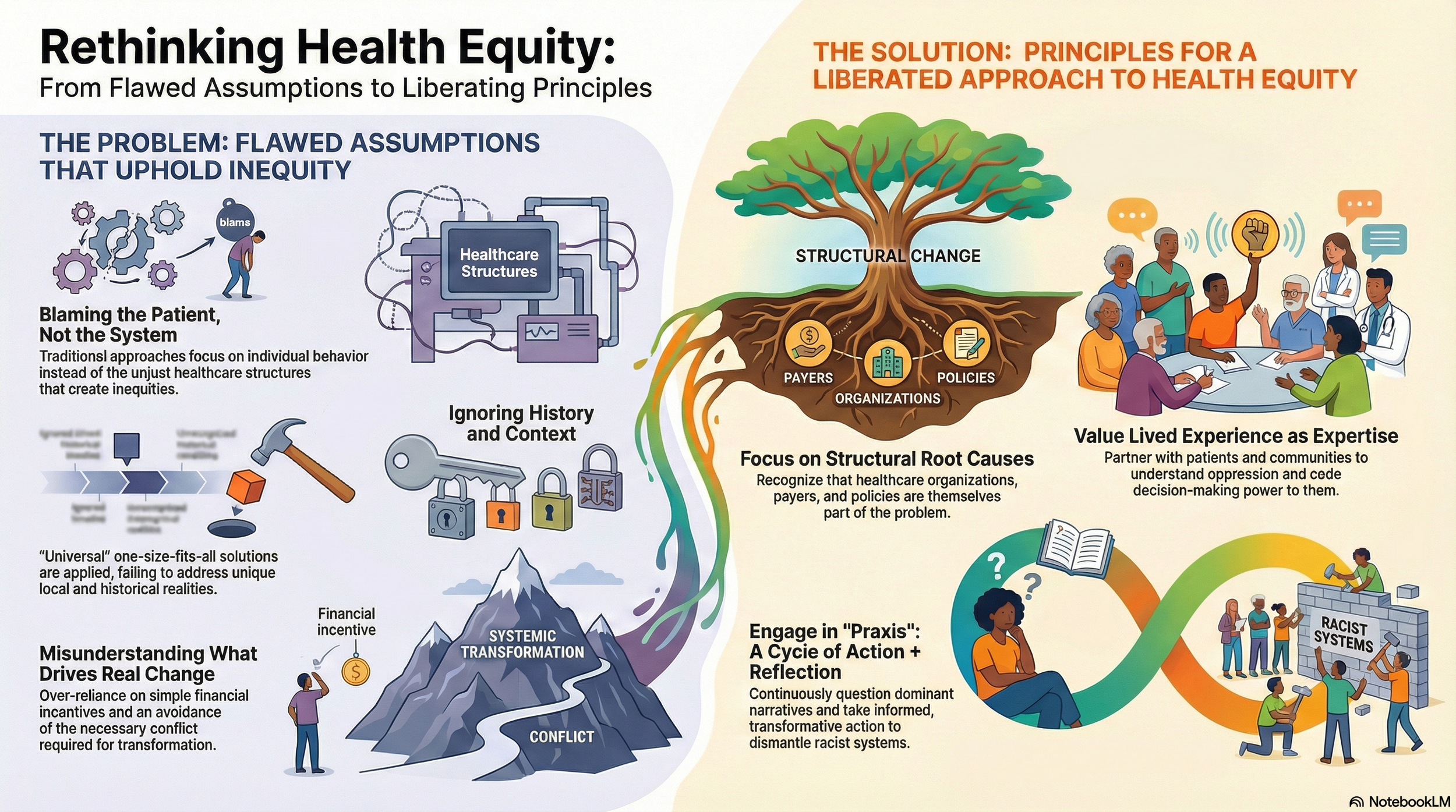
1. We're Asking the Wrong Questions—And Blaming the Wrong People
A core barrier identified by the program is an ideological assumption the researchers, citing liberation psychology, call individualism. Western psychology and healthcare have a powerful tendency to frame systemic problems at the individual level. We instinctively focus on the person experiencing the inequity rather than the system causing it, which subtly shifts the blame and leads to ineffective solutions.
The program found a powerful example of this in its own early work. Consider the difference between these two questions about asthma hospitalization rates:
• The typical question: "Why do Black children with asthma have higher rates of hospitalization than white children with asthma?"
• The better question: "Why is our health system less successful helping Black children with asthma avoid hospitalization than white children with asthma?"
The first question frames the problem around the children and their families, implying the cause lies with them. The second question correctly frames the problem as a failure of the health system. This shift is critical. The program’s systematic reviews revealed that this flawed framing is widespread; most interventions inadvertently reinforced the bias that patients needed fixing, and were designed to change them instead of the providers, organizations, or policies that were failing them.
--------------------------------------------------------------------------------
2. We Mistake Harmony for Progress
In most professional settings, harmony, consensus, and equilibrium are seen as signs of a healthy team. However, when tackling deeply rooted issues like racism, this "homeostatic vision"—the assumption that disequilibrium and discord are inherently negative—becomes a major obstacle to progress.
The program learned that addressing the root causes of health inequity requires difficult conversations that inevitably stir powerful feelings—not just frustration or anxiety, but also defensiveness and confusion. Avoiding this friction to maintain a sense of harmony is not a sign of progress; it is a sign of avoidance.
According to the lessons learned, this disequilibrium should be reframed as a positive sign of progress. The temporary discord that arises when directly confronting issues of power and racism is a necessary, generative, and transformative part of creating real change. Individuals and teams need support to see this discomfort not as a problem to be solved, but as evidence that the real work is finally beginning.
--------------------------------------------------------------------------------
3. We Apply "Universal" Fixes to Unique, Historical Problems
Another flawed assumption is ahistoricism—the belief that models and solutions are universal and can be applied across different cultures and historical contexts without modification. This "one-size-fits-all" approach ignores the unique circumstances that create inequities in the first place.
The program’s analysis points out that most of our healthcare and psychological science is based on the experiences of European Americans. These models are then applied universally, often leading to less effective prevention, screening, and care for people of color. The work of liberation psychologist Ignacio Martín-Baró highlights the danger of this mindset:
"models created in different circumstances from our own, and assumed to be cross-cultural and transhistorical, can lead to a serious distortion of what our peoples are really about"
This insight forces us to abandon generic solutions and instead commit to the work of recovering historical memory—understanding the unique political, social, and economic forces that created and sustain the problem in a specific community.
--------------------------------------------------------------------------------
4. We Were Afraid to Name the Real Problem
For years, the national program—despite its mission—was reluctant to directly name the primary driver of the inequities it was trying to solve: racism. The term "structural racism" was not referenced in its public documents or guidance.
Initially, the program even favored the term "disparities" over "equity." While measuring disparities is a crucial metric, this focus avoided a social justice or antiracism framework. As the researchers later concluded, it was a power-neutral approach to a problem rooted in power, which ultimately limited the program's thinking and the scope of its solutions.
The turning point came with the stark realities exposed by the COVID-19 pandemic and the public outrage over police brutality. This crystallized the need for the program to finally center antiracism in its work and explicitly name racism as a root cause. The lesson was profound: progress is impossible until we are willing to identify, name, and directly confront the true source of the problem.
--------------------------------------------------------------------------------
Conclusion: To Change the System, First Change the Mind
The 17-year journey of this national program reveals a crucial truth: our most significant barriers to achieving health equity are not just technical or financial, but psychological and ideological. The biggest hurdles are often our own unexamined assumptions about individuals, conflict, history, and even the language we use.
The framework of "liberation psychology" helped the program's leaders uncover these faulty assumptions and chart a new course. Their 17-year journey of action and reflection—of praxis—challenges us to look inward. If these hidden beliefs can stall a well-funded effort in healthcare, what deeply ingrained assumptions might be quietly sabotaging progress in your own work and life?